
Which Exercises “Load” the Supraspinatus Most?
May 14, 2026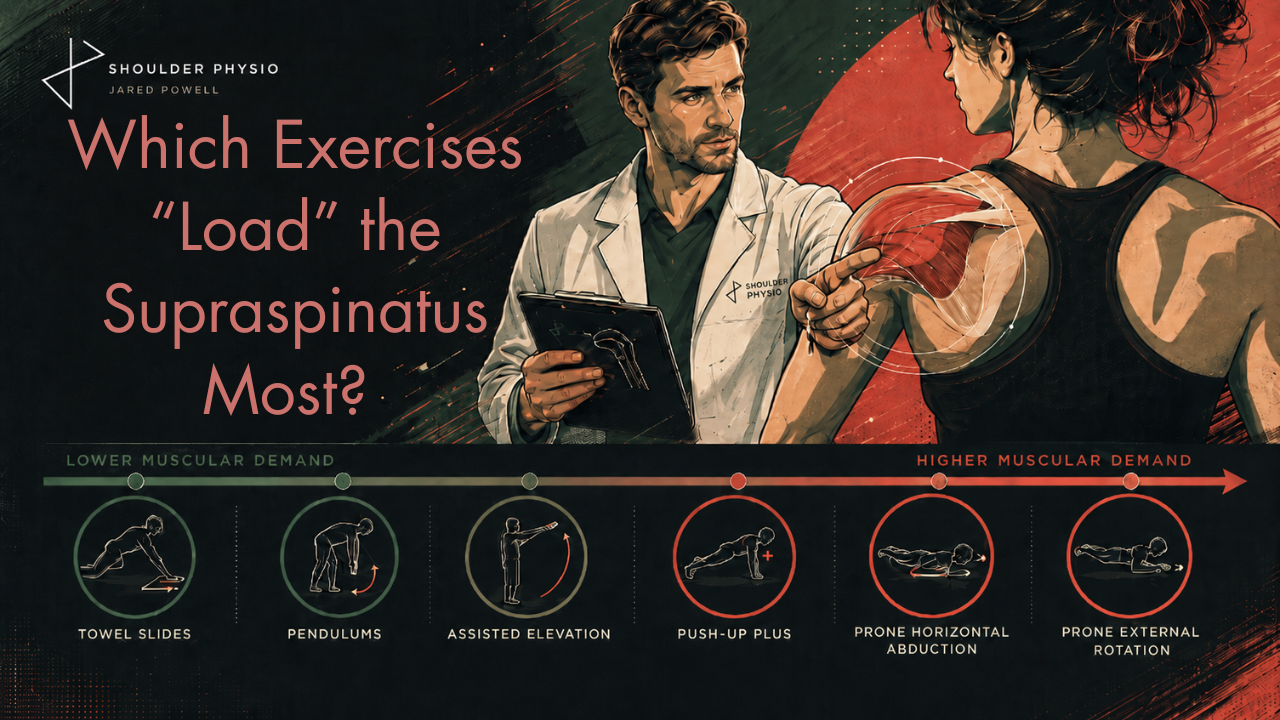
A common consideration in the rehabilitation of MSK injuries is to what extent do various exercises “load” or “activate” particular muscles and tendons. The terms are often used somewhat loosely, particularly in online discourse, where exercises are criticised for "barely activating" the glutes, VMO or multifidus. You get the idea. The underlying theory is that specific activation of particular muscles is important for successful rehabilitation.
I’m not a huge fan of this philosophy in general, but in some contexts, such as rehabilitation after surgery, understanding the relative muscular demands associated with different exercises may be useful. In the context of post-operative supraspinatus repair rehabilitation, for example, what exercises are a safe place to start, and which ones may expose healing tissue to substantially greater demand?
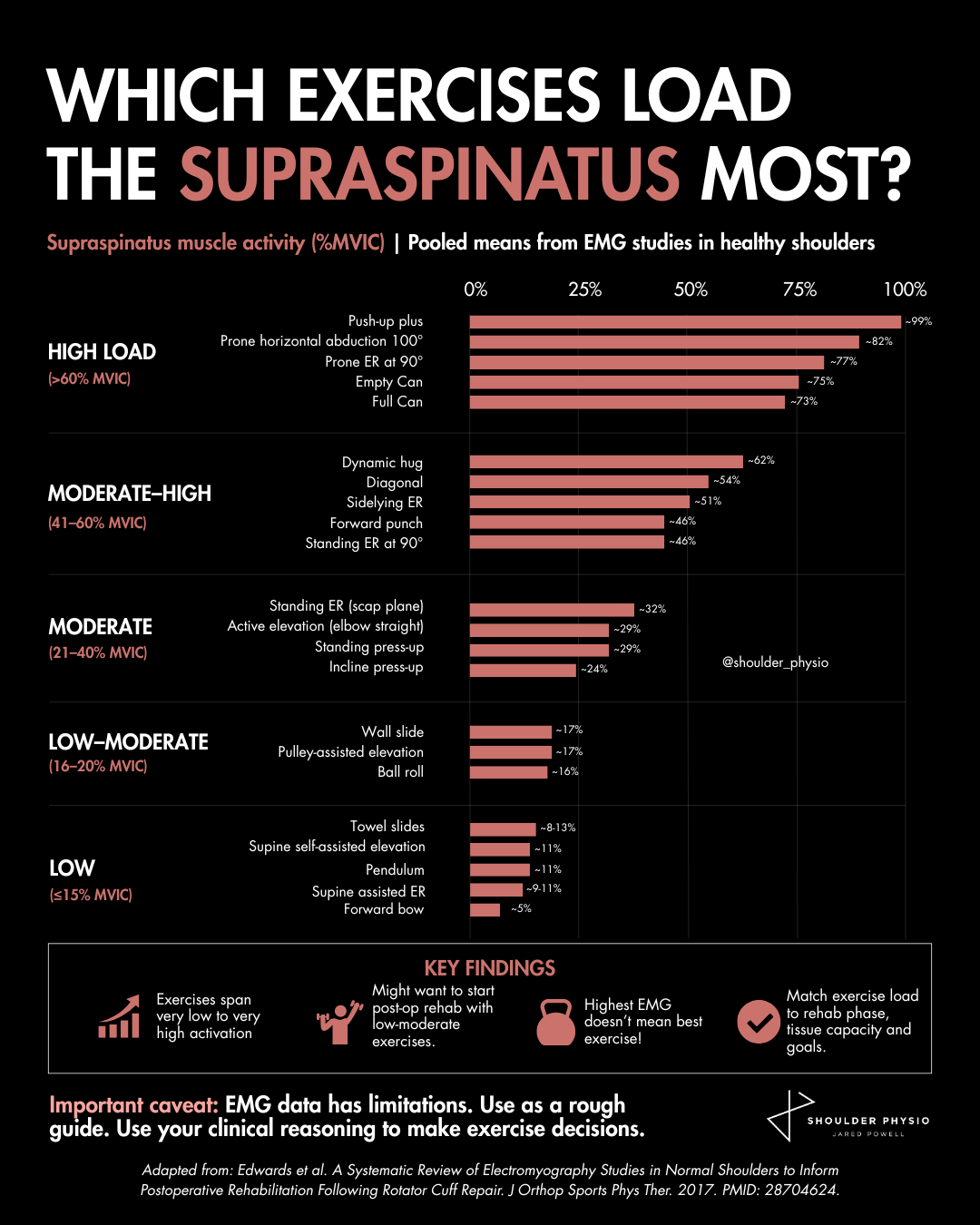
A wonderful systematic review by Edwards et al. pooled electromyography (EMG) data from 20 studies to examine supraspinatus muscle activity during common shoulder rehabilitation exercises. The findings make interesting reading, and I will attempt to summarise it for you in this blog (with a little bit of nuance too).
Exercises such as the push-up plus, prone horizontal abduction, and prone external rotation generated very high EMG amplitudes, while towel slides, pendulums, and assisted elevation drills sat at the opposite end of the spectrum. Hopefully, this makes sense and is not surprising data.
It is tempting to interpret this as a leaderboard of “best” exercises. Higher EMG must mean a better exercise, right? Not so fast. EMG studies can be clinically useful, particularly in postoperative rehabilitation where clinicians may wish to expose healing tissues to progressively greater loads over time. In the context of a rotator cuff repair, knowing that a pendulum exercise likely imposes substantially lower muscular demand than a push-up plus can help guide sensible early-stage exercise selection. This is especially relevant during the first weeks and months after surgery when repair integrity may still be vulnerable.
But problems begin when we mistake EMG amplitude for a direct measure of exercise quality, tendon load, or clinical value.
EMG offers a window into neuromuscular excitation, but only a partial window. It does not directly measure tendon force, tissue stress, adaptation, recovery, or clinical effectiveness. High EMG amplitude does not necessarily equal high tendon load or superior rehabilitation outcomes.
In fact, the review itself repeatedly acknowledges the limitations of interpreting EMG data in isolation. Different studies used different normalisation procedures, different electrode placements, and different exercise techniques. The same exercise performed differently can produce very different outputs. Even the terminology we use requires some caution. Strictly speaking, EMG measures electrical activity associated with muscle excitation, not “muscle activation” or “load” directly. Forgive me for the clickbait title in the figure above.
Perhaps more importantly, rehabilitation is not ultimately about “activating muscles.” It is about restoring people to meaningful movement and valued activities.
Patients do not simply want a supraspinatus that fires harder on EMG. They want to sleep comfortably, return to work, lift their child, swim again, throw again, or train again. Muscles do not exist in isolation from tasks, goals, confidence, adaptation, and context.
The question is not simply:
“Which exercise activates the supraspinatus most?”
but:
“Which movement best helps this person move forward?”
This is why I think we should be cautious about becoming overly muscle-centric in rehabilitation. EMG evidence can absolutely inform rehabilitation. It can help us appreciate relative muscular demands and guide exercise progression, particularly after surgery. But it should remain a guide, not a destination.
Reference
Edwards et al. A Systematic Review of Electromyography Studies in Normal Shoulders to Inform Postoperative Rehabilitation Following Rotator Cuff Repair. J Orthop Sports Phys Ther. 2017. PMID: 28704624.
The Complete Clinician
Tired of continuing education that treats clinicians like children who can’t think for themselves?
The Complete Clinician was built for those who want more.
It’s not another lecture library, it’s a problem-solving community for MSK professionals who want to reason better, think deeper, and translate evidence into practice.
Weekly research reviews, monthly PhD-level lectures, daily discussion, and structured learning modules to sharpen your clinical edge.
Join the clinicians who refuse to be average.

