
The rotator cuff tear... Information for clinician and patient alike
Aug 12, 2019
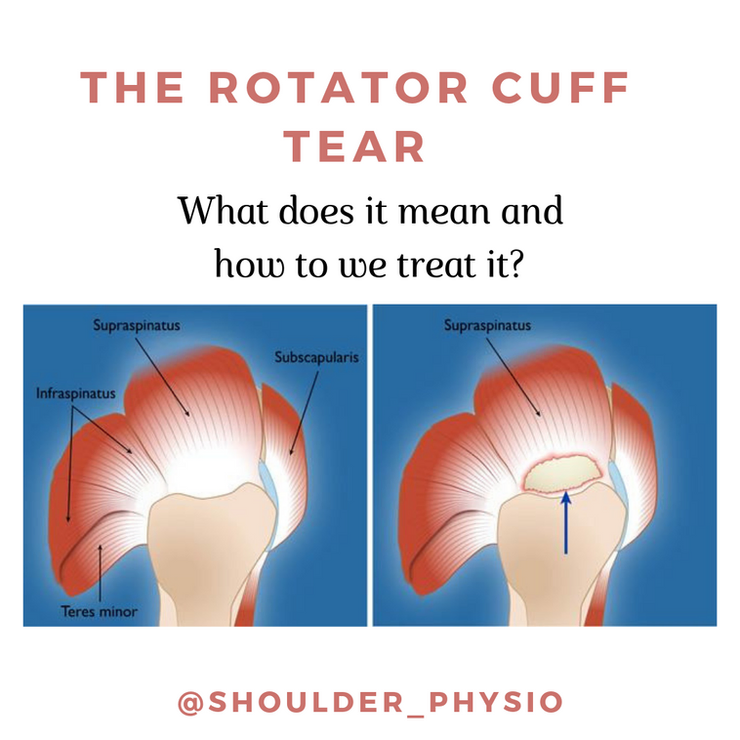
The holy grail of shoulder pain. Pain related to the rotator cuff will be evident in up to 80% of people who present with a painful shoulder. In many of these cases, a tear will be evident on ultrasound or MRI. What does this mean exactly? A tear/abnormality can be further sub-divided into:
- Tendinopathy/tendonitis
- Partial thickness tear
- Full thickness tear
- Subacromial bursitis often accompanies all of the above
Age is the biggest risk factor for developing a rotator cuff tear. In fact, there is a decade-on-decade rise in the prevalence of rotator cuff tear after the age of 40. In addition, overuse, underuse, occupation, smoking, genetics, and general health (thyroid, diabetes, high blood pressure, high cholesterol, obesity) are all associated with increased risk of rotator cuff tear. Some of these we can't change (genetics, age) but some (lifestyle factors - smoking etc.) we certainly can!
The location, size, and progression of tear size are relevant factors for prognosis. In addition, the mechanism of injury, age of the patient, presence of fatty infiltration can also impact on recovery. Not all rotator cuff tears are equal! Treat it on a case by case basis. Also, please remember to actually physically assess somebody, treat the wo(man) not the scan. We will not dive into psychosocial factors in this short piece.
Most rotator cuff tears can be managed effectively via conservative measures, namely physical therapy with a focus on progressive resistance training. Physical therapy should be given at least 12 weeks of progressive, challenging, and informative therapy. The only exception I will make here is a full-thickness rotator cuff tear that is sustained in a traumatic fashion (i.e. falling over) that measures >1cm. This group should get an opinion from an orthopaedic surgeon, if that is what they desire.
Partial-thickness, small atraumatic full thickness tears, and especially tendinopathy/bursitis must be subjected to a trial of exercise therapy first. The evidence firmly states that 80% of people with such pathology can be successfully managed with a 12 week progressive exercise regime targeting the shoulder.
A note on injections. This includes corticosteroid and platelet rich plasma (PRP) injections. DO NOT pursue these as a first line intervention. There is minimal robust evidence suggesting long term effectiveness of either. In fact, exercise therapy is more effective than PRP injections (Nejati, 2017). Corticosteroid injection can be useful, but when studied systematically, they tend to help only 20% of people more than a placebo! (Mohamadi, 2017).
Exercise therapy (progressive resistance training) is the gold standard first line intervention for rotator cuff tears. What type of exercise, how often, how heavy, and how much pain is allowed are the big questions here. In short, there is no consensus regarding this. Something is better than nothing. It should be tailored to the individual to align with wants, needs and goals. It should be stimulating and challenging and accessible to aid compliance. It should be progressive (increasing weight, reps, ROM) and relevant to the individual.
See your physiotherapist for more information (make sure they are up to date and evidence-based!).
The Complete Clinician
Tired of continuing education that treats clinicians like children who can’t think for themselves?
The Complete Clinician was built for those who want more.
It’s not another lecture library, it’s a problem-solving community for MSK professionals who want to reason better, think deeper, and translate evidence into practice.
Weekly research reviews, monthly PhD-level lectures, daily discussion, and structured learning modules to sharpen your clinical edge.
Join the clinicians who refuse to be average.

