
God, give me strength!
Jun 07, 2021
Unsurprisingly the bulk of the name calling and mudslinging took place on twitter. Twitter is a social media platform capable of so much good, but often poisoned and ruined by misrepresentations, personal attacks, and invidious conduct by otherwise good people (on all sides of the relevant debate). What is it about twitter that seems to promote this outrage culture more than other platforms? I’m not entirely sure, but it certainty vindicates my decision to spend a very small portion of my life on it.
The purpose of this commentary is to provide (to the very best of my ability) a balanced account of the latest furore than has engulfed our profession (physiotherapy).
Now, we all have biases, and I will declare mine here;
I love strengthening. I love strengthening for MSK rehabilitative purposes. I love strengthening for general health and well being purposes. I love strengthening for its myriad positive secondary benefits. I love strengthening for my own clinical practice and exercise pursuits (I have been lifting iron for 20 years). I love strengthening for its clinical and cost-effectiveness. I love strengthening. I also believe there is much more to pain, especially persistent pain, than strength and getting stronger. We could probably end the blog here, but in trying to avoid the ever present straw man, more needs to be said.
In the April 2021 issue of the JOSPT I published a paper titled “Rotator Cuff–Related Shoulder Pain: Is It Time to Reframe the Advice, “You Need to Strengthen Your Shoulder”? (ref). This Viewpoint paper has a very clear and simple premise (well I thought it did). In brief, the paper articulates, in 1500 words, how shoulder mechanics (including strength, scapular kinematics, and muscle timing and activity) MAY not need to substantially change or improve for a general improvement in pain and function to occur, for RCRSP. This appears true across many bodily locations and pathologies:
Now, somehow this message has been interpreted (either maliciously or naively), as being a gross attack on the prescription of strengthening exercise for rehab purposes and, astonishingly, an attack on clinicians who advocate strengthening exercise. This is totally befuddling. Worse. Its an egregious assault on honesty and fact. The paper actually waxes lyrical about the value of resistance exercise and strongly concludes that it should be used as part of a holistic rehab regimen for RCRSP. If you would like to read the paper and you can’t get access – please email me and I can assist so you can think for yourself.
In addition to this, a clinical trial titled; “Effectiveness of Adding a Large Dose of Shoulder Strengthening to Current Nonoperative Care for Subacromial Impingement” by Clausen et al 2021 (ref) has recently been published. Predictably, this has caused a stir. I commend the authors for conducting such a rigorous pragmatic clinical trial that has real world clinical implications. I will not review the paper because its already been done to death on social media with differing levels of prudence. The paper simply concludes that adding a large dose of shoulder strengthening exercise to normal guideline care for what the authors call ‘subacromial impingement’ is no more effective than guideline care alone. The results of this paper DO NOT suggest that strengthening exercise is ineffective. Strengthening exercise were part of both groups clinical care package and both groups improved, equally, according to the SPADI. The usual care could have included any or all of the following interventions:
- Advice
- Strengthening
- Stretching
- Manual therapy
- Massage
- Acupuncture
- Electrotherapy
So, we can conclude the heterogenous mix of ‘usual care’ was just as effective as ‘usual care + an additional dose of strengthening exercises’. We just don’t know the individual role each intervention played in the causing the clinical outcomes. Was it the strengthening that helped? Stretching? Massage and manual therapy? Even bloody electrotherapy? Its unclear. So, no firm conclusion can be made on the efficacy of each intervention. For more information on the difference between an efficacy and effectiveness trial see my recent Instagram post (ref).
An interesting finding of this trial is the almost complete absence of change in shoulder strength in both groups. Now there are myriad reasons that could account for this, including: pain, exercise dosage, adherence to exercise regimen, equipment used, and infinite other person level factors (including fear and catastrophic beliefs etc.). Despite the lack of change in shoulder strength (for whatever damn reason) there was a clinically important improvement in shoulder function in both groups (ref). We can speculate, based on this, that a substantial improvement in shoulder strength is not required to observe a clinically important improvement in shoulder function. Whilst this was not the aim of this study, it sure is an interesting adjunct feature of the paper, and one that requires further investigation (I am in the process of doing this!).
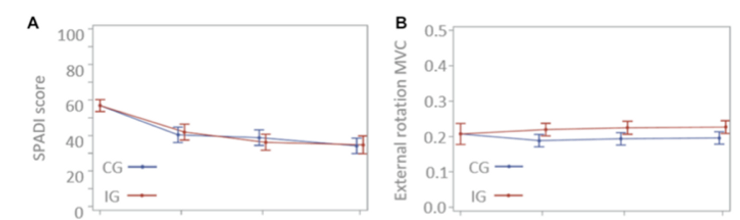
Ref: Clausen et al 2021
To be clear, this does not mean that we should not pursue an increase in shoulder strength. It seems intuitively correct to me if we identify shoulder weakness in a person with shoulder pain that we should attempt to change this (I am very aware about the limited utility of intuition). However, in attempting to change the measure of shoulder weakness, we must accept that we are influencing the individual in ways the go far beyond the ability of the shoulder to produce force. In fact, I state this very clearly in my paper; “Exercise (including resistance exercise) may have a hypoalgesic effect, improve health-related quality of life, improve pain-related self-efficacy and confidence, influence systemic inflammatory markers, mark time while nature takes its course, provide a distraction, and potentially lead to a re-evaluation of pain” (ref)
I hope I have clearly conveyed my thoughts here. All ideas are fair game to be challenged. This applies to surgery, injection therapy, electrotherapy, acupuncture, manual therapy, stretching and even strengthening! A problem emerges, I think, when ideas and beliefs become so definitive, entrenched and absolute that any attempt to question, challenge, or even engage in dialogue on said ideas is perceived as a personal attack. Changing these beliefs becomes akin to undergoing a religious conversion, its damn near impossible. I will finish with a quote from Karl Popper;
“All knowledge is provisional, temporary, capable of refutation at any moment”.
Thanks and I will see, talk, interact with you soon :)
Jared
The Complete Clinician
Tired of continuing education that treats clinicians like children who can’t think for themselves?
The Complete Clinician was built for those who want more.
It’s not another lecture library, it’s a problem-solving community for MSK professionals who want to reason better, think deeper, and translate evidence into practice.
Weekly research reviews, monthly PhD-level lectures, daily discussion, and structured learning modules to sharpen your clinical edge.
Join the clinicians who refuse to be average.

